Vaccines offer the best hope for ending the COVID-19 pandemic.
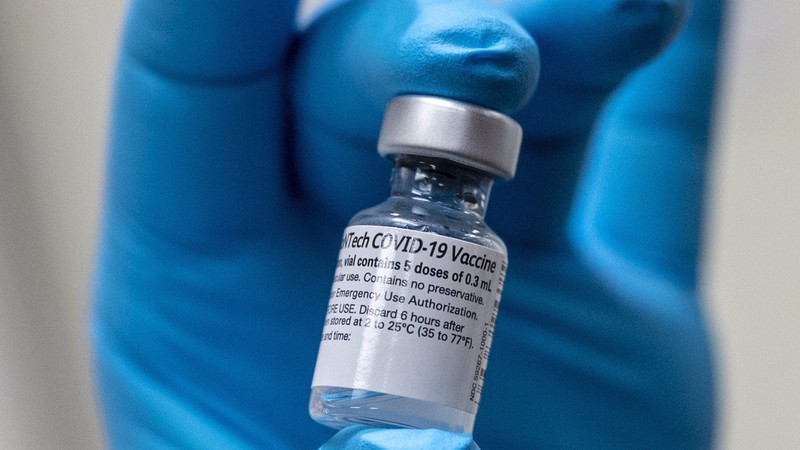
With multiple COVID vaccines now available, here are the differences and similarities. U.S. Defense Department / Wikimedia Commons CC BY 2.0
UPDATE: The federal Food and Drug Administration on Oct. 20 updated its authorizations of all three COVID-19 vaccines in use in the United States to allow for “booster” doses of each, for specific groups. A “booster” shot is an additional dose of a vaccine given to reinforce the protection against a specific disease offered by an initial vaccination.
The immunity produced by vaccines, including the COVID-19 vaccines, decreases as time passes. Booster shots bring the lowered level of protection back up. In September, the FDA authorized booster shots of the COVID vaccine manufactured by Pfizer-BioNTech, but only for people age 65 and over, as well as people as young as 18 who are deemed to be “at high risk of severe COVID-19."
The FDA also included people over 18 whose jobs put them at high risk of contracting the COVID-19 virus in their Pfizer authorization. That group includes health care workers, prison employees, grocery store workers, schoolteachers and others whose work puts them in close proximity with people who may be infected.
On Oct. 20, the FDA also authorized booster shots of the Moderna vaccine for those same groups. The agency also authorized a booster shot of the Johnson and Johnson vaccine for anyone age 18 or over who initially received the J&J shot. The J&J vaccine required just one shot initially. People vaccinated with the single-dose shot are eligible for a booster just two months after their first shot, the FDA decided.
Recipients of the Moderna and Pfizer vaccines which require two doses must wait at least six months before getting a booster, according to the FDA authorization.
The FDA also, for the first time, will allow “mix and match” vaccines—meaning that recipients of any brand of COVID vaccine may receive a booster shot of any of the other authorized brands.
_________
The first real hope to finally end the nine-month-old coronavirus pandemic in the United States arrived on Dec. 11, 2020, when the federal Food and Drug Administration gave the green light to a vaccine manufactured by the pharmaceutical industry giant Pfizer, and the German firm BioNTech. Within the next two weeks, about 3 million doses of the two-dose vaccine were shipped throughout the country—including about 550,000 to California.
A week after approving the Pfizer vaccine, the FDA did the same for a similar vaccine against the SARS-CoV-2 virus developed by the 10-year-old, Massachusetts-based biotech company Moderna, with the federal government planning to deliver shipment totaling about 5.9 million doses across the country. Gov. Gavin Newsom announced that 670,000 of those Moderna doses would be shipped to California.
Two months after that, on Feb. 27, the FDA gave the green light to a third COVID-19 vaccine, this one manufactured by Johnson & Johnson. The administration of President Joe Biden quickly announced that it would immediately distribute 4 million J&J doses across the country, to pharmacies and community health centers, and to states.
Time to celebrate! Right? The end of the grueling, deadly pandemic which (at that time in mid-March) had killed more than 540,000 Americans—at least 54,000 of them Californians—was now in sight.
Needless to say, the situation was not that simple. While the arrival of not one but two vaccines against the fast-spreading, potentially lethal virus does did indeed offer the best hope for bringing the state, country and, for that matter, the world back to something resembling a pre-COVID state of “normalcy,” a long, often grim and rocky road was still ahead. Managing public expectations and hopes would be one of the most important factors in smoothing that road as much as possible.
So what do we need to know about the vaccines, in order to best understand the possibilities they offer, or don’t offer? Let’s start with the basics.
What Is a Vaccine?
Simply put, a vaccine is a medication that causes your body to produce an immune response to a particular disease without ever giving you the disease. That way, if you are ever exposed to said disease, your immune system fights it off, and you don’t get sick or die. Until recently, vaccines accomplished this remarkable feat because they were made from a dead, or significantly weakened, version of the very pathogen, or germ, they were designed to immunize against.
Newer vaccines, including the three new COVID vaccines and others still in testing but not yet federally approved, operate differently, the particulars of which we will discuss shortly.
While the mid-20th century was the golden age of vaccine development, with vaccines for such childhood scourges as polio, measles, mumps and rubella all created within a less than a couple of decades, from the mid 1950s to the late 1960s, the practice of vaccination is not a new phenomenon. According to the College of Physicians of Philadelphia’s History of Vaccines website, an early type of inoculation against smallpox was employed in China more than 1,000 years ago.
The modern era of vaccination began in 1796 when an English doctor named Edward Jenner made the observation that milkmaids who had previously contracted a nasty, but not fatal, skin infection known as cowpox appeared to be immune to the far more lethal disease, smallpox. The process by which he turned that insight into a vaccination probably wouldn’t pass muster today. He injected an eight-year-old boy with the fluid from lesions on the hands of a cowpox-infected dairy maid.
The boy got sick for about a week, but fully recovered. At that point, Jenner injected the lad with potentially deadly material taken from a smallpox pustule. But the boy did not die. In fact, he did not get sick at all. The two-century process of eradicating smallpox from the planet had begun.
How Are COVID Vaccines Different?
The technology that allowed the first two approved COVID-19 vaccines to be developed in a few short months, rather than many long years, is also what makes them potentially more effective and reliable than traditional inoculation vaccines, as described above. This biotech is called mRNA, or “messenger RNA,” and was first tested in 1990. In fact, one of the initial pair of vaccine-makers takes its name from mRNA—from 2010 to 2018, the company called itself ModeRNA Therapeutics, before opting for the shorter, catchier “Moderna.”
Since 1930, the most common method for manufacturing vaccines was to let a virus or bacteria grow, multiplying by the billions. Eventually, scientists would extract these mass-produced pathogens and weaken or kill them, enabling them to be used safely for purposes of vaccination. For the majority of those vaccines, the chosen incubator for growing the pathogens was chicken eggs.
Even now, at research and pharmaceutical facilities across the United States, millions upon millions of eggs are stored to be used for the purpose of growing germs. The flu vaccine, which needs to be updated every year due to the rapidly changing characteristics of the viruses that cause influenza, accounts for most of that egg use. About 82 percent of all flu vaccines are egg-based.
But the novel coronavirus that causes COVID-19 cannot grow in eggs. Which works out well, because mRNA vaccines do not require eggs. In fact, mRNA does not require “growing” at all. The Pfizer and Moderna mRNA vaccines are created entirely by chemical means in a laboratory. No eggs or organic material involved.
According to a Harvard Medical School summary, mRNA vaccines use strands of artificially created genetic material that exactly duplicate the genetic structure of, not an entire virus, but just one part of the virus’s “protein coat.” Any virus is essentially nothing more than a packet of nucleic acid—that is, the genetic materials DNA or RNA—wrapped in protein.
The mRNA vaccines, rather than using the entire virus (albeit a disabled version), simply use a snippet of genetic material to trick the body’s immune system into firing up a defensive response to a virus that isn’t even there. The single strand of RNA is delivered to cells in a package of microscopic globs of fat.
Once delivered, the immune system believes it has detected the coating of the coronavirus and starts pumping out antibodies, rendering a vaccine recipient immune to the actual virus itself.
The Centers for Disease Control explains that “mRNA vaccines do not contain a live virus and do not carry a risk of causing disease in the vaccinated person.”
In addition, “mRNA from the vaccine never enters the nucleus of the cell and does not affect or interact with a person’s DNA.” So no worries about being turned into a genetic mutant.
What’s the Difference Between the Pfizer and Moderna Vaccines?
Both Pfizer and Moderna created their vaccines with mRNA technology, but there are some differences between the two. Both vaccines require two separate doses to achieve their maximum effectiveness. The second dose of the Pfizer vaccine is supposed to be administered 21 days after the initial injection. Moderna vaccine recipients must wait 28 days. After both doses, the effectiveness of the two vaccines is similar, and surprisingly high: 94.1 percent for Moderna, per the Food and Drug Administration; 95 percent for Pfizer.
But differences in effectiveness begin to show up over varying age groups, at least for the Moderna vaccine. While Pfizer’s vaccine in its clinical trials showed consistent efficacy in recipients from ages 16 to 89, Moderna’s saw a significant dropoff for patients over age 65, for whom the vaccine’s efficacy came in at 86.4 percent. Still impressive, but more than nine points below the 95.6 percent effective rate in the 18-64 age range.
The two vaccines also showed a notable difference in efficacy after just the first dose. In trials, one dose of the Pfizer vaccine proved just 52.4 percent effective. Moderna did much better with a single dose, coming in at 80.2 percent efficacy.
Perhaps the most important difference between the two mRNA vaccines is how they are stored—an important detail because it affects the ease, or difficulty, in distributing each vaccine. Each dose of the Pfizer vaccine must be stored, and transported, at the ultra-frigid temperature of 94 degrees below zero Fahrenheit. The Moderna doses can be kept in a normal refrigerator, anywhere between 36 and 46 degrees, which lets them keep for 30 days.
In February, however, the FDA relaxed its requirements for ultra-cold storage of the Pfizer vaccine. Under the new standards, the FDA allowed the vaccine to be stored at standard refrigeration temperatures for up to two weeks.
The two vaccines are not compatible. A patient whose first dose comes from Pfizer should not complete the program with a Moderna shot—and vice versa.
What’s the Story With Johnson & Johnson?
The third approved vaccine, Johnson & Johnson, is created—and functions—differently from the initial two. J&J’s vaccine uses a double strand of DNA, rather than a single one of RNA, to deliver its immune system-triggering mechanism. Rather than using fat as a coating for the genetic material, the DNA is packed inside an adenovirus—basically a common cold virus, but one that has been rendered inactive.
When the adenovirus enters a human cell, the DNA inside tells the cell to produce the mRNA needed to create an immune response to stave off an infection by the SARS-CoV-2 coronavirus.
The adenovirus technology has a couple of advantages over the mRNA vaccine method. First, because DNA is more stable than RNA, the doses do not require ultra-cold storage. Second, and even more important, an adenovirus sets off an immune response powerful enough that only one dose of the stuff is needed. No need for a second appointment to get a booster shot.
But the J&J vaccine also comes with an apparent disadvantage. In global, clinical trials, the adenovirus-based vaccine proved to have just 66 percent efficacy, compared to the much higher numbers posted by the two mRNA vaccines. But when it came to preventing serious cases of COVID-19, and deaths from the disease, J&J performed much better in the trials, at about 85 percent efficacy.
Experts have been careful to note, however, that the J&J clinical trials were conducted under different conditions than the Pfizer and Moderna trials, making direct comparison difficult. One significant difference: the J&J trials were conducted later, after several variant strains of the virus had emerged.
Now may be a good time to make an important point: There is a big difference between “efficacy” and “effectiveness.” The term “efficacy” refers to how well a vaccine performs in a clinical trial, comparing a large set of vaccinated subjects with a control group made up of non-vaccinated people.
In other words, if the non-vaccinated group experienced 100 COVID infections, but the vaccinated group saw only five, then the vaccine is said to have 95 percent efficacy.
“Effectiveness” is the term used to describe how a vaccine performs in the real world. The first, wide-reaching “real world” study of a vaccine’s effectiveness was conducted in Israel, where scientists tracked 596,618 people who received the Pfizer vaccine between December and February.
The Pfizer vaccine’s real-world effectiveness closely matched its clinical efficacy numbers. Seven days after receiving the second dose of the Pfizer vaccine, the vaccinated people had 94 percent fewer symptomatic COVID cases than an unvaccinated group of the same size. Of the nearly 600,000 vaccinated people in the study, only nine died of COVID-19 after being fully vaccinated, compared to 32 of the unvaccinated individuals studied.
The Johnson & Johnson 'Pause'
The Johnson & Johnson vaccine hit a roadblock on April 13, 2021, when the CDC and Food and Drug Administration “paused” its use after a small number of J&J recipients turned up with an uncommon type of blood clot. At the time, out of approximately eight million people who got the J&J shot, six developed cerebral venous sinus thrombosis, a type of clot that affects between two and five people out of every every million people each year. So, a rare one. But one not normally associated with vaccines.
After an investigation that took 10 days, the CDC and FDA gave authorization for the Johnson & Johnson vaccine to resume being administered to Americans. By then, the health agency had found just 28 cases of the blood clots, all in patients younger than 60, with women from ages 30 to 39 years old accounting for the largest segment of the 28. Three of the patients died, but 19 had been discharged from the hospital by May 7. But given the rarity of the clots compared to the millions who had received the shot, the health agencies decided that the benefits of using the J&J COVID vaccine far outweighed the risks.
 Subscribe
Subscribe

